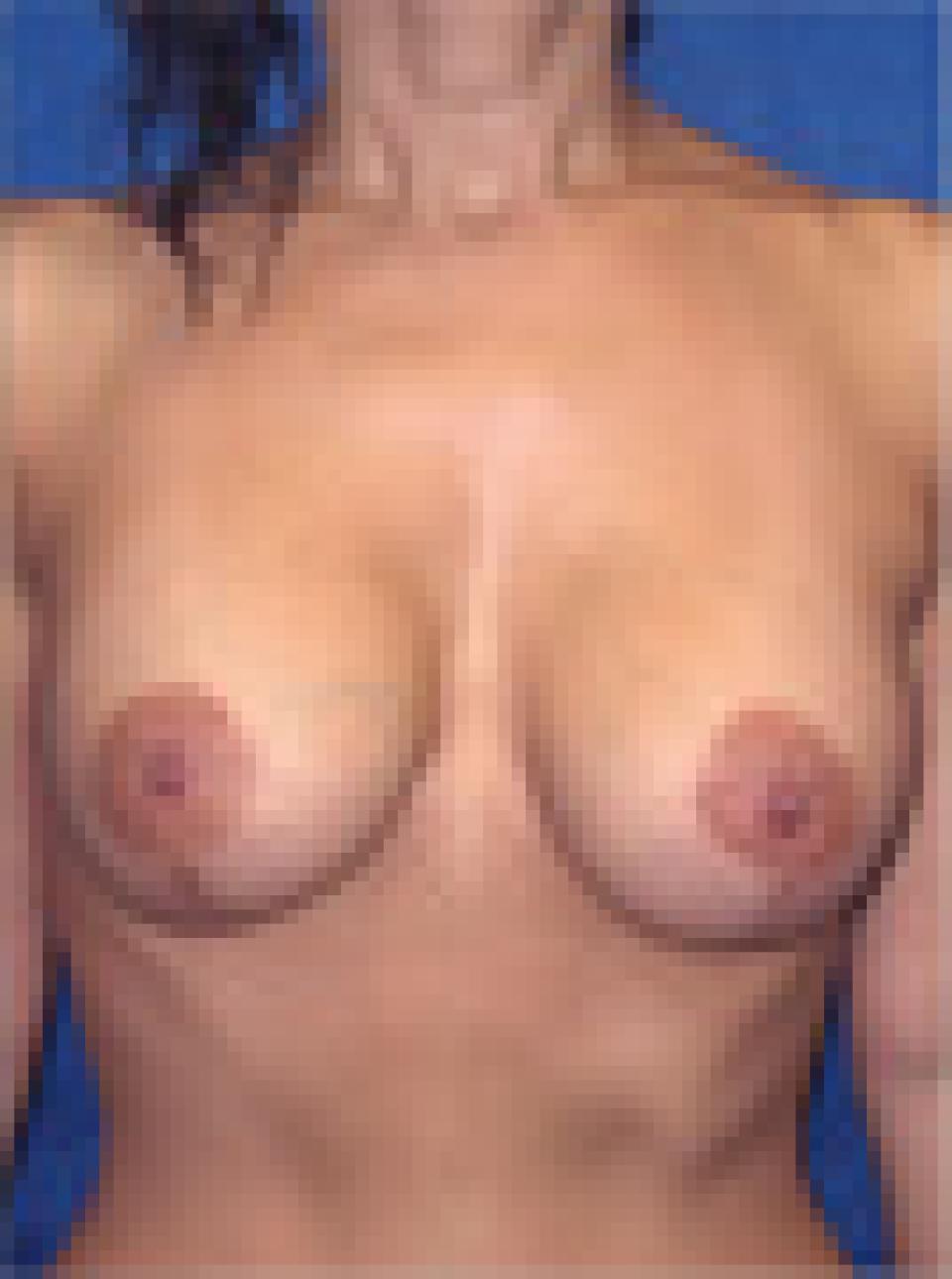
This 31 year old woman underwent breast reduction in which approximately one and one third pounds of tissue was removed from the right breast and almost two pounds of tissue was removed from the left breast.
In this individual’s case, the incisions used to perform the breast reduction were of the “lollipop” or short scar type. This method of breast reduction avoids any incisions in the cleavage and in most instances along the lower fold of the breast.
This woman, like many others, had noticeably asymmetric breasts. In her case, the left breast was noticeably larger than the right breast. I make every effort to correct this during surgery, but ultimately, no two sides look identical after surgery- just as they did not before surgery.
Also very visible in this individual are the "shoulder grooves" from her bra straps. This is a common issue in women who have extremely large breasts or "macromastia." The pressure from the bra straps typically cause pain, open wounds and sometimes even numbness and tingling in one or both hands from compression of the underlying nerves. Breast reduction can alleviate these symptoms almost instantaneously.