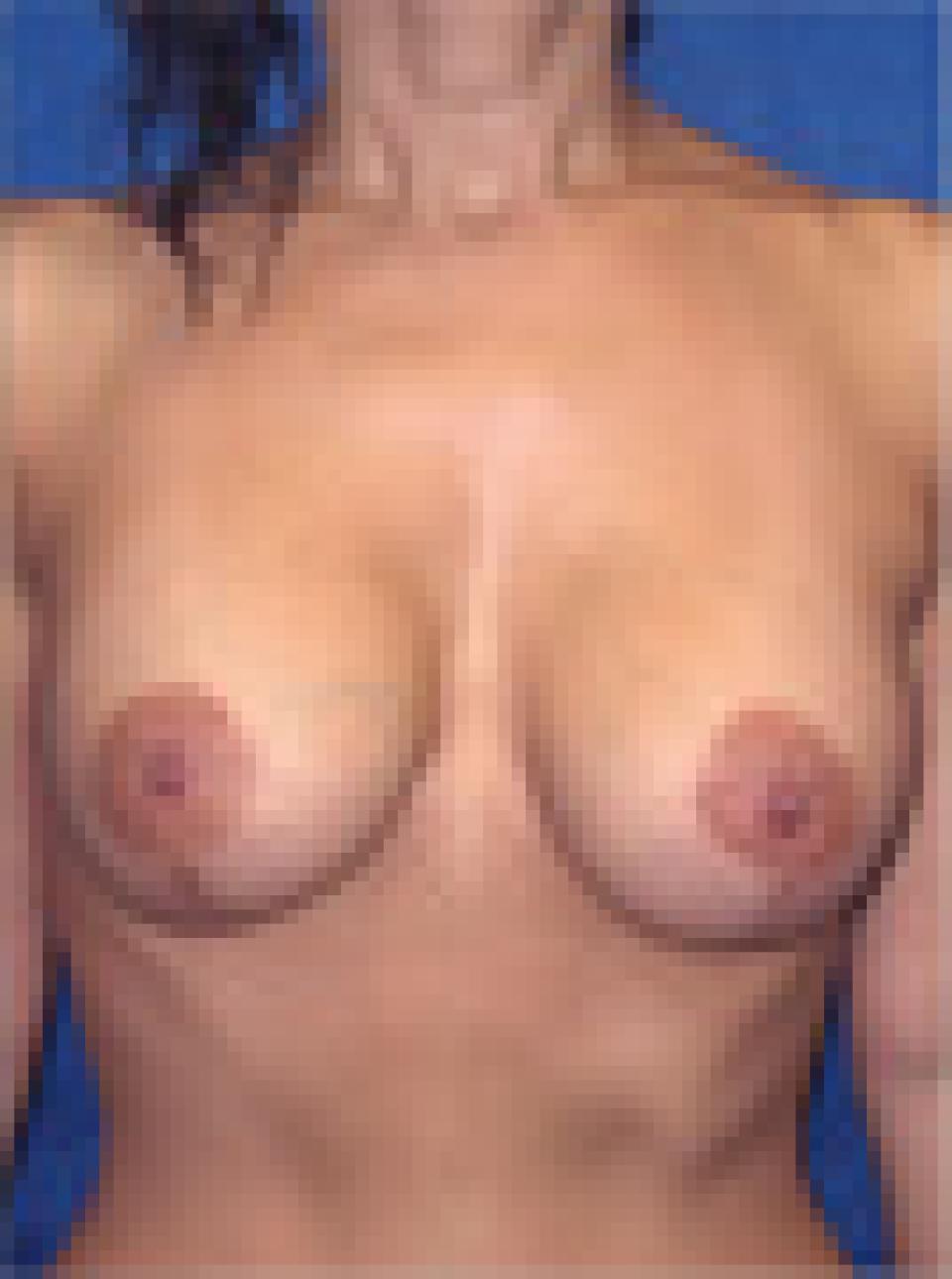
When it comes to deciding what approximate breast size you wish to achieve, the best advice I can give you is that you should be guided by your physical frame. Indeed, you may in fact be limited by it. In my practice, I select implants based upon your chest measurements, the quality of your breast skin and the size of your breasts prior to surgery.
I perform breast augmentation through a peri-areolar or inframammary approach and I place that vast majority of implants at least partially beneath the pectoralis muscle. My patients are welcome to select either saline or silicone filled breast implants. Silicone filled implants can in some cases achieve a more natural feel and may be a particularly attractive option for women with less breast tissue prior to surgery.
More >>
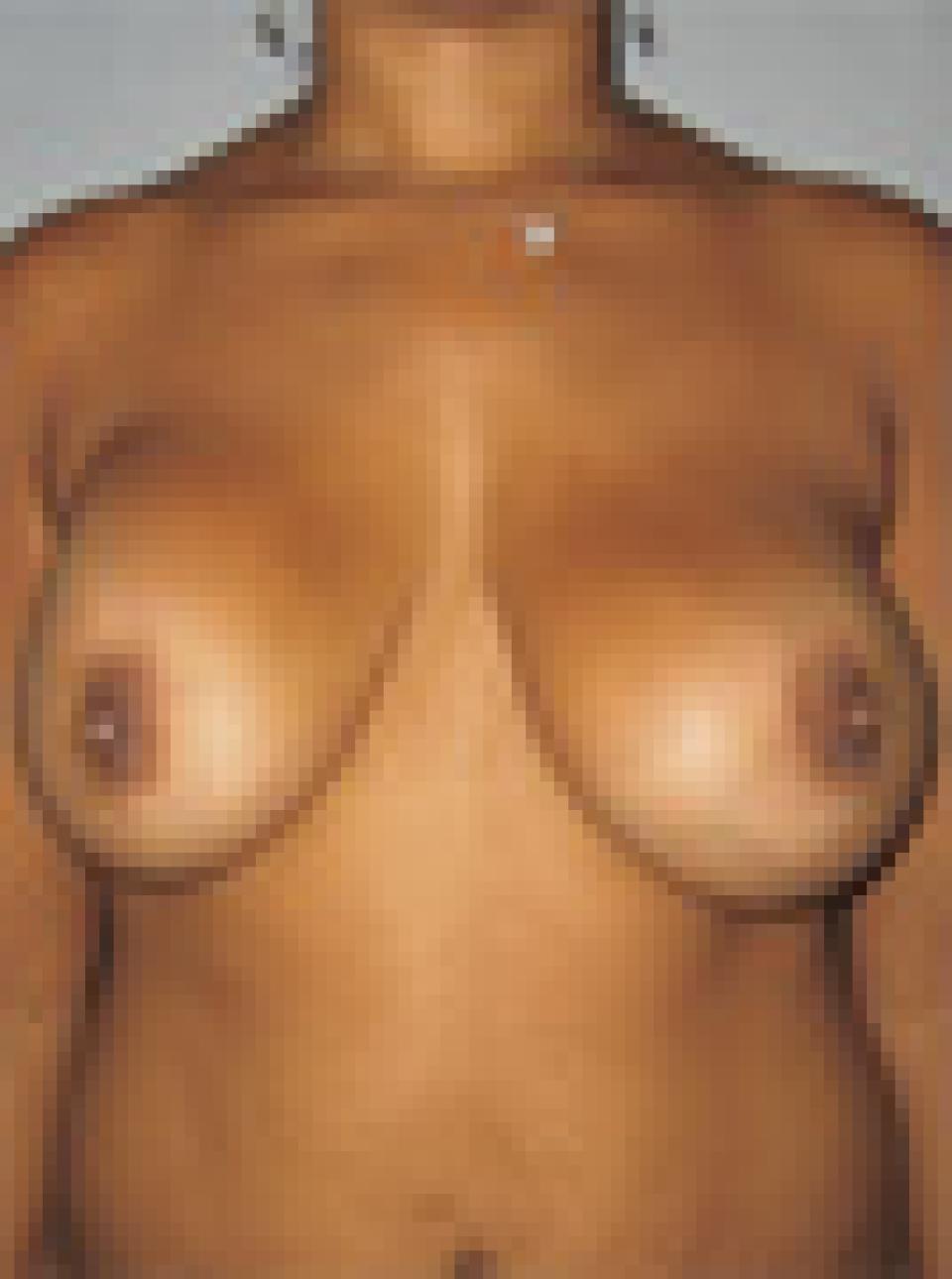
In my practice, I perform breast lifts using incisions that result in a “lollipop” shaped scars. With good care and a bit of luck, these incisions heal well and the scars are difficult to see from a distance. Nevertheless, a woman who undergoes a cosmetic breast lift must be prepared for scars that are visible. This is one example of a “trade-off” in plastic surgery and of course, there are many others. This is one, however, that I feel is more than worthwhile in appropriate candidates.
More >>
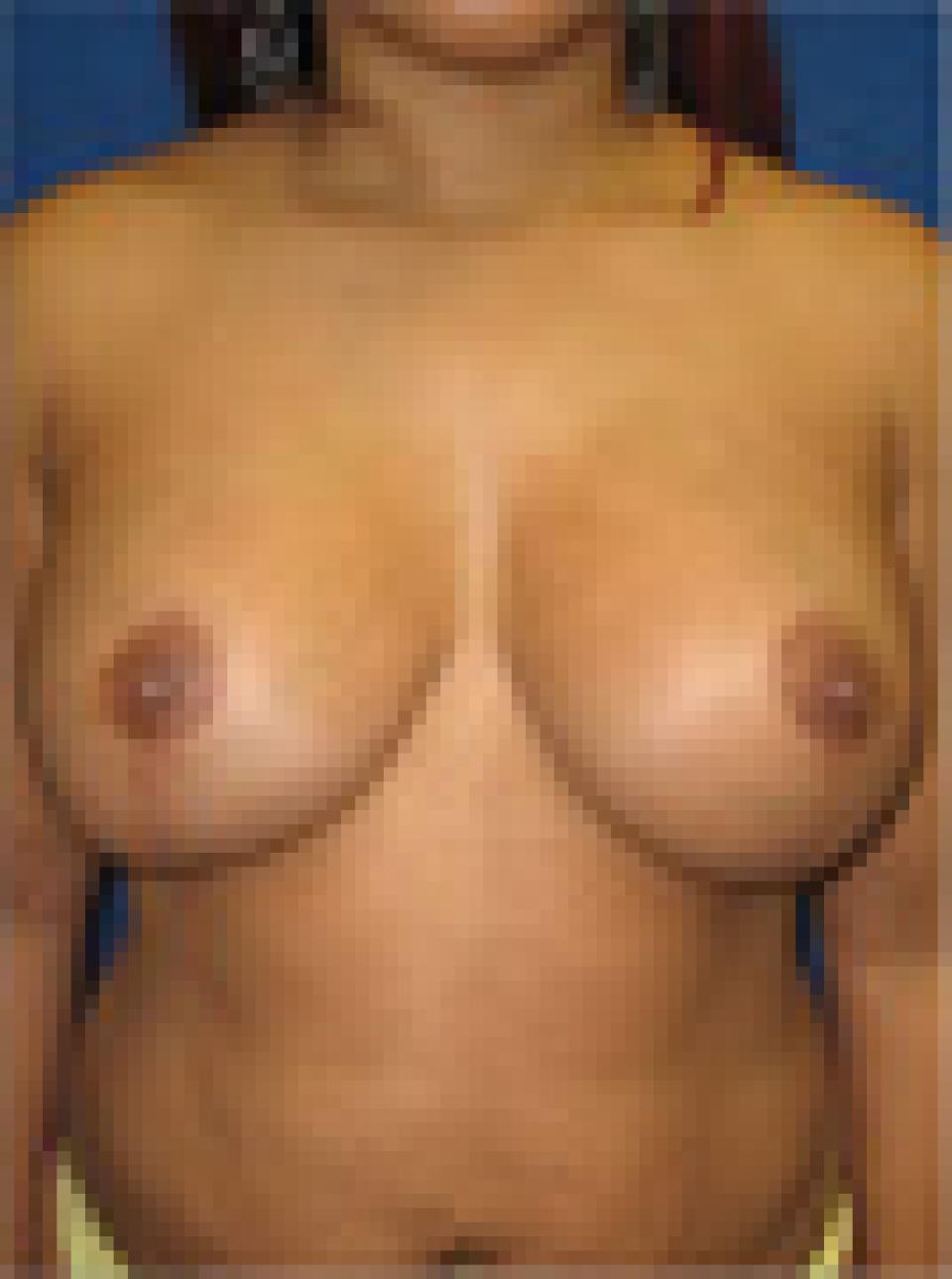
I apply the same criteria to patients who have had their surgery elsewhere as I do to my own patients. I am typically reluctant to re-operate on a breast augmentation patient for minor issues, because each time one undergoes revision, many of the risks of surgery tend to be multiplied. This is why I spend a great deal of time discussing size preferences and the likely outcome of surgery with my patients pre-operatively. It is said frequently that the most common reason for re-operation of the breasts in women who have had breast augmentation surgery is that they wish to “go bigger.” Ultimately, I feel that this is a poor reason to undergo repeated surgical procedures that can only result in more scar tissue, which is unpredictable, and thinning of the native tissues, which are necessary to cover the implant and provide a natural looking result. I encourage patients to think carefully about the risks of revision in cases where there is not a major problem.
More >>