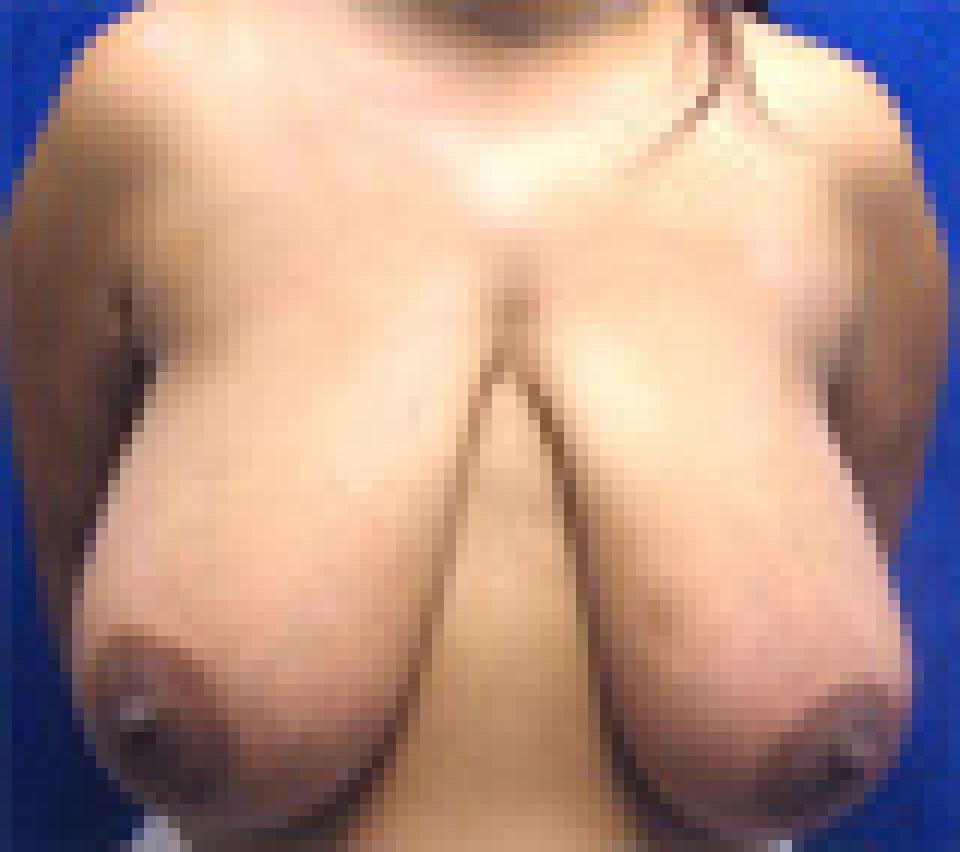
This 26 year old woman reached her plateau weight after losing 74 pounds following bariatric surgery. She had a breast lift or mastopexy using a technique which leaves behind scars in the shape of an “anchor.”
In some patients who lose a large amount of weight, the natural end point of the breast laterally disappears and the breast appears to continue around towards the back. This is what has happened to this woman.
In selected individuals who have this problem, the “anchor” scar type breast lift can be amended to remove that skin excess on the side of the body beneath the arm. This is the reason that I selected that particular breast lift technique in this woman even though the scars that it leaves behind are longer and more difficult to conceal in a swimsuit.
Looking at her photographs after surgery, it is obvious that there is no longer a "wing" of skin that continues laterally towards the back. Instead, the breast has a round shape and ends as it typically does before the side of the body that lies beneath the arm.
Unfortunately, there is now a visible scar there. This is an example of what I refer to as a “trade off” in plastic surgery. It is important to decide what is more important to each individual patient- a scar or better contour. Sometimes, it is not possible to have both!