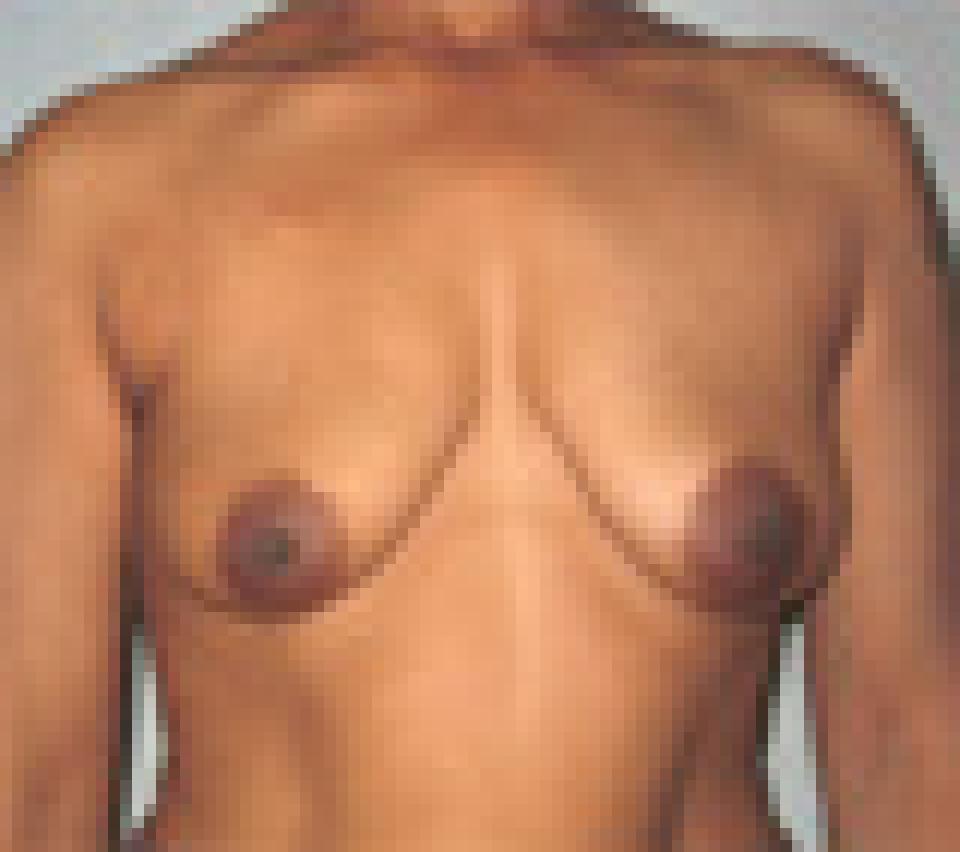
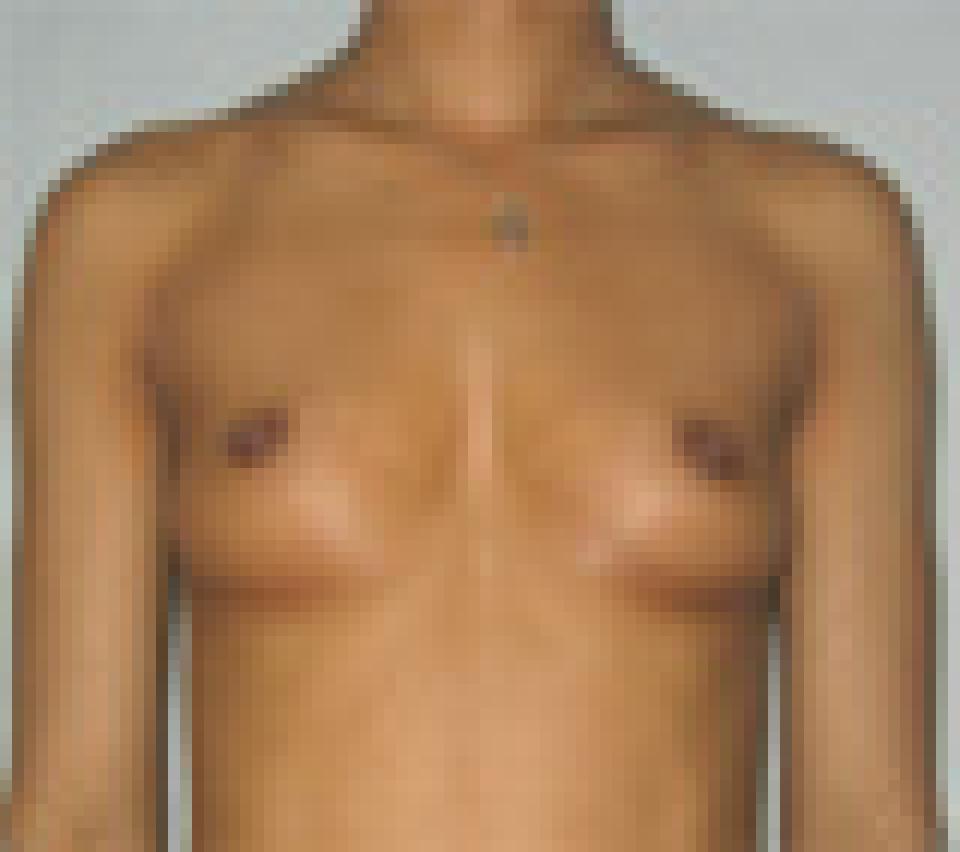
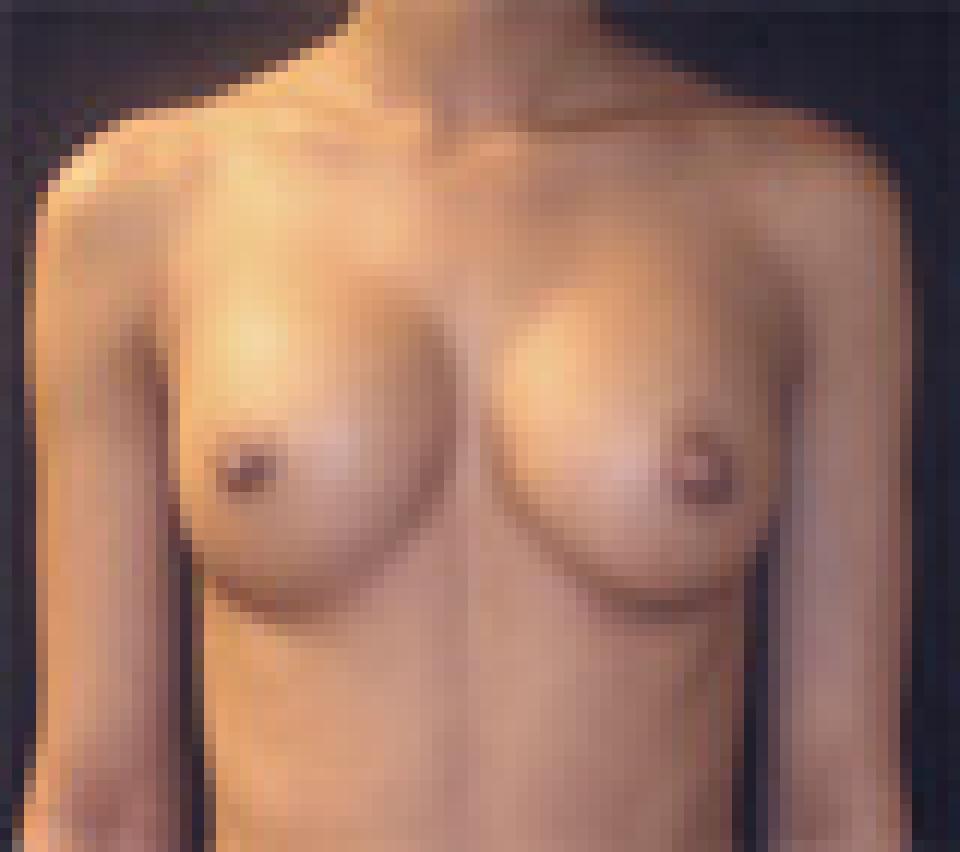
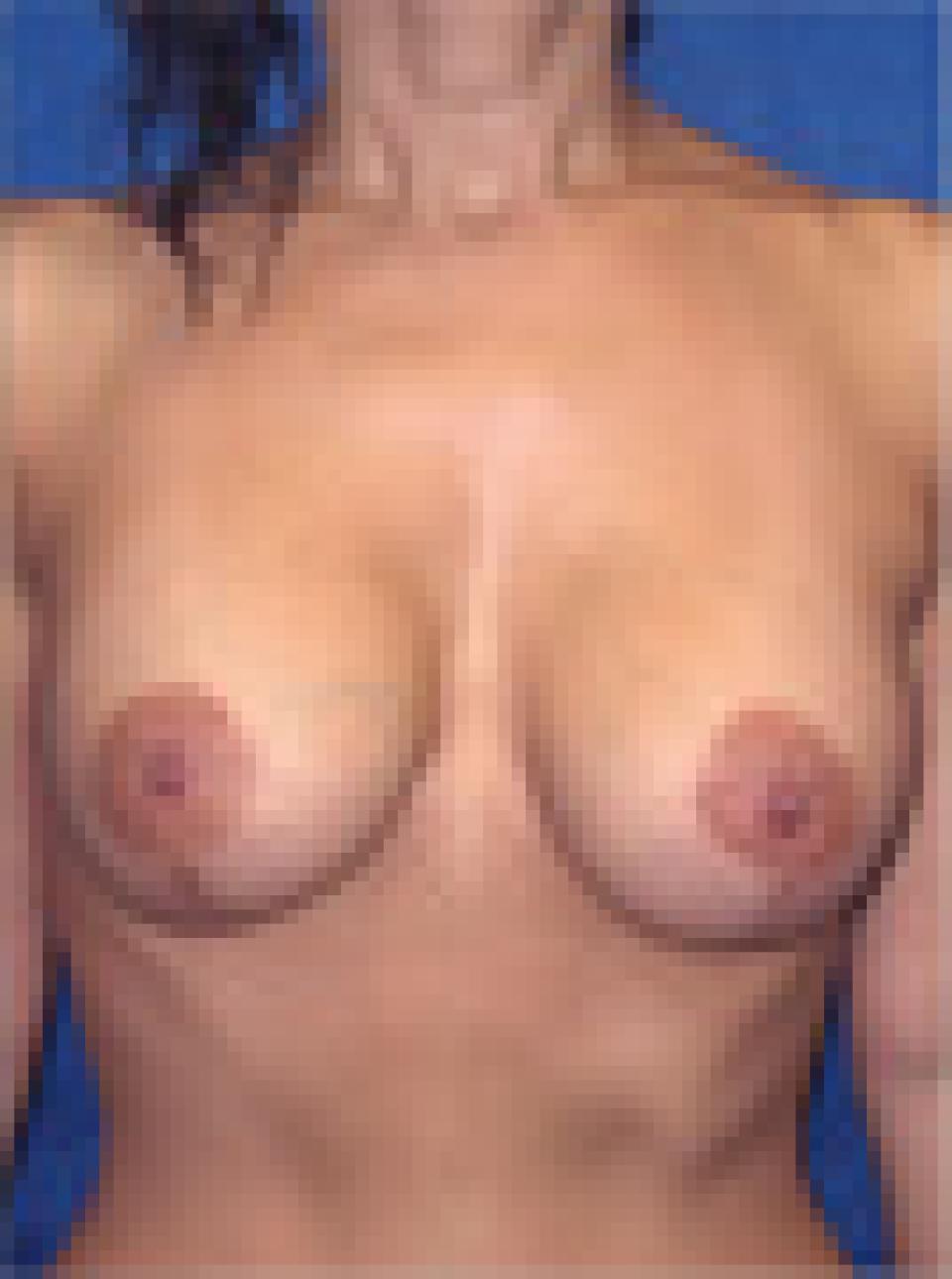
This 32 year old woman underwent breast augmentation using saline filled breast inflated to a volume of 195 cc’s and placed partially beneath the pectoralis muscle.
The individual has a mild pectus excavatum, a condition in which a person's breastbone is sunken into the chest. She also has a tendency to stand in a slightly kyphotic position, which means that her upper back is rounded and her head is relatively forward.
Obtaining a natural looking result in a patient who has pectus excavatum and postural abnormalities, as this individual has, can be challenging but is certainly possible.
In the case, the implants were inserted through a 3 cm incision at the lower border of the areola, which is the darker skin surrounding the nipple. These incisions typically heal quite well and can be difficult to see.