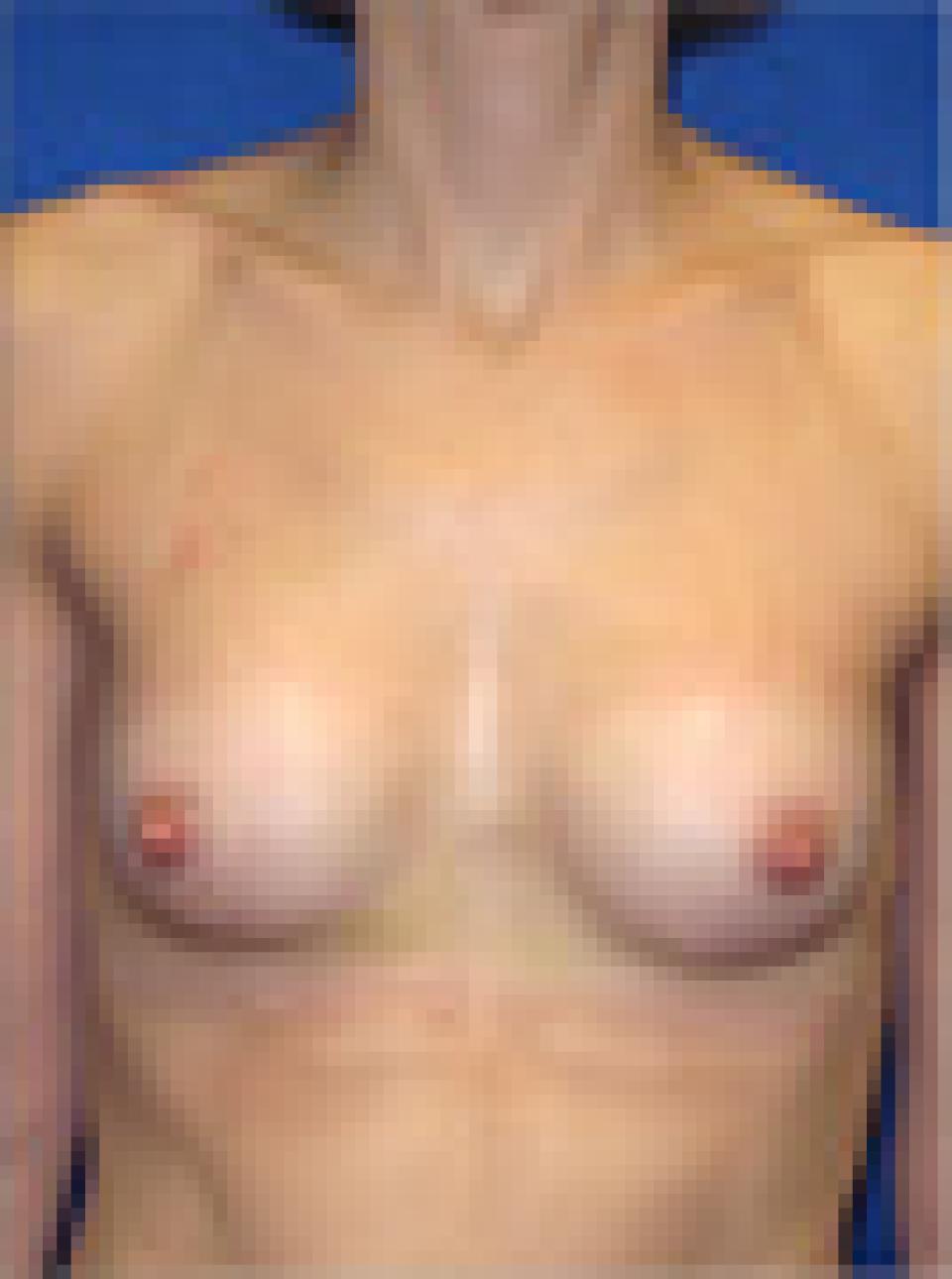
This 30 year old woman underwent breast augmentation using 180 cc silicone filled breast implants placed partially beneath the pectoralis muscle through an incision along the lower fold of the breast that measured 3 centimeters in length.
Implants can also be inserted through an incision on the edge of the areola, which is the dark colored skin surrounding the nipple. However, when an individual has very small areolas, such as this patient has, this is not possible.
On the other hand, if the areolas are too large or irregularly shaped, they can be resized and reshaped at the same time as a breast augmentation and/or a breast lift is performed. This will, however, result in a scar around the periphery of the new areola. Often, these scars can heal quite well and are less objectionable in their appearance than overly large or irreguarly shaped areolas.