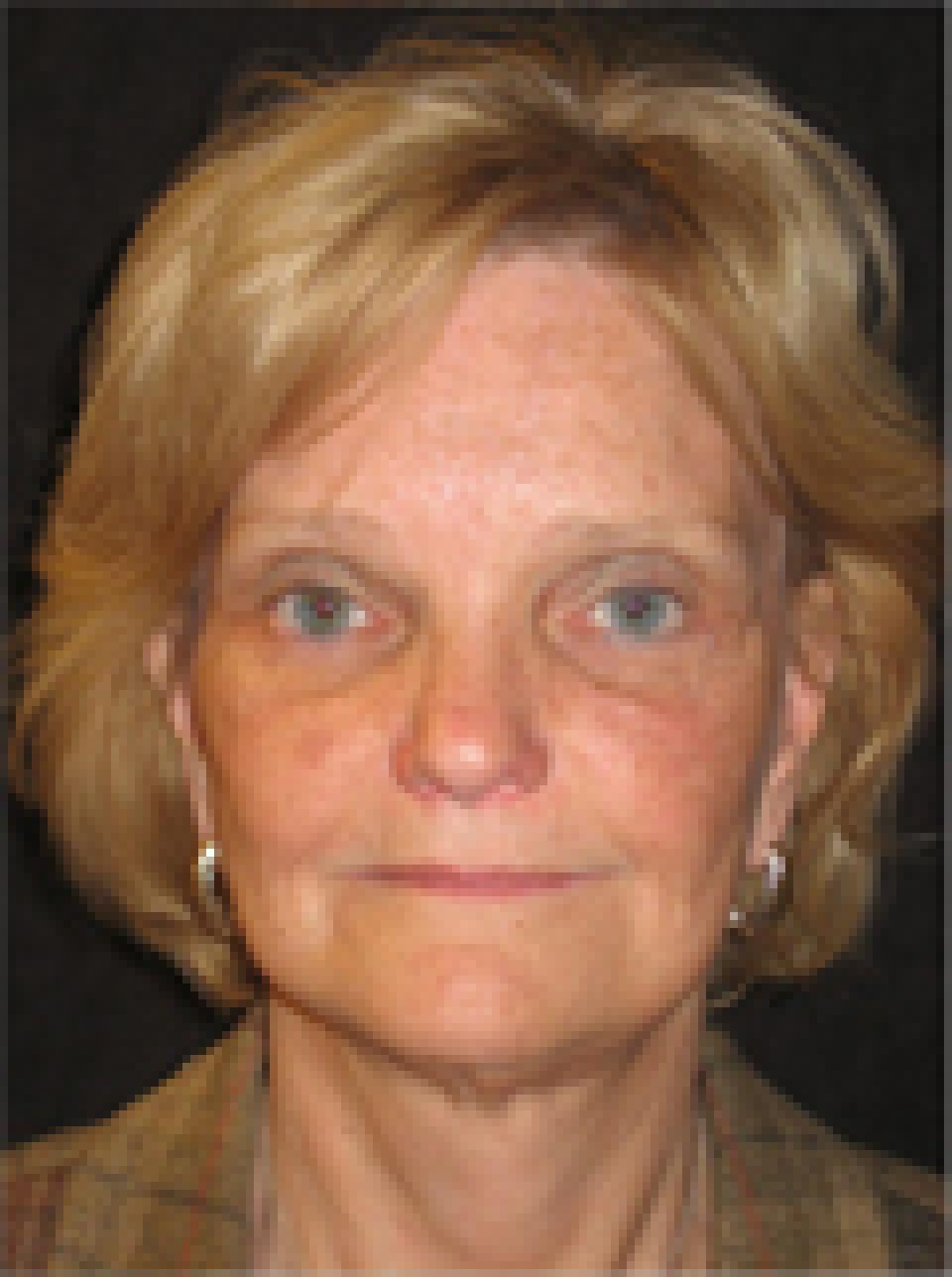
This case depicts a 56 year old woman who wished to improve the appearance of sagging skin that she had developed as a result of age and dramatic weight loss.
She underwent an endoscopic brow lift, upper and lower eyelid lifts, a short scar face lift and a neck lift. Her post-operative photographs depict her appearance at approximately 4 months after surgery.
Although a properly executed short scar face lift can effect some improvement in the appearance of sagging skin in the neck with no incisions behind the ears, individuals with an extensive amount of skin and muscle descent require longer incisions and a formal neck lift to achieve dramatic results.